🎬 Video Lesson Available
Watch the full 7-slide video lesson for Respiratory System with AI teacher narration and visual explanations.
01The Bio-Energetics of Respiration: Fueling Cellular ATP Production

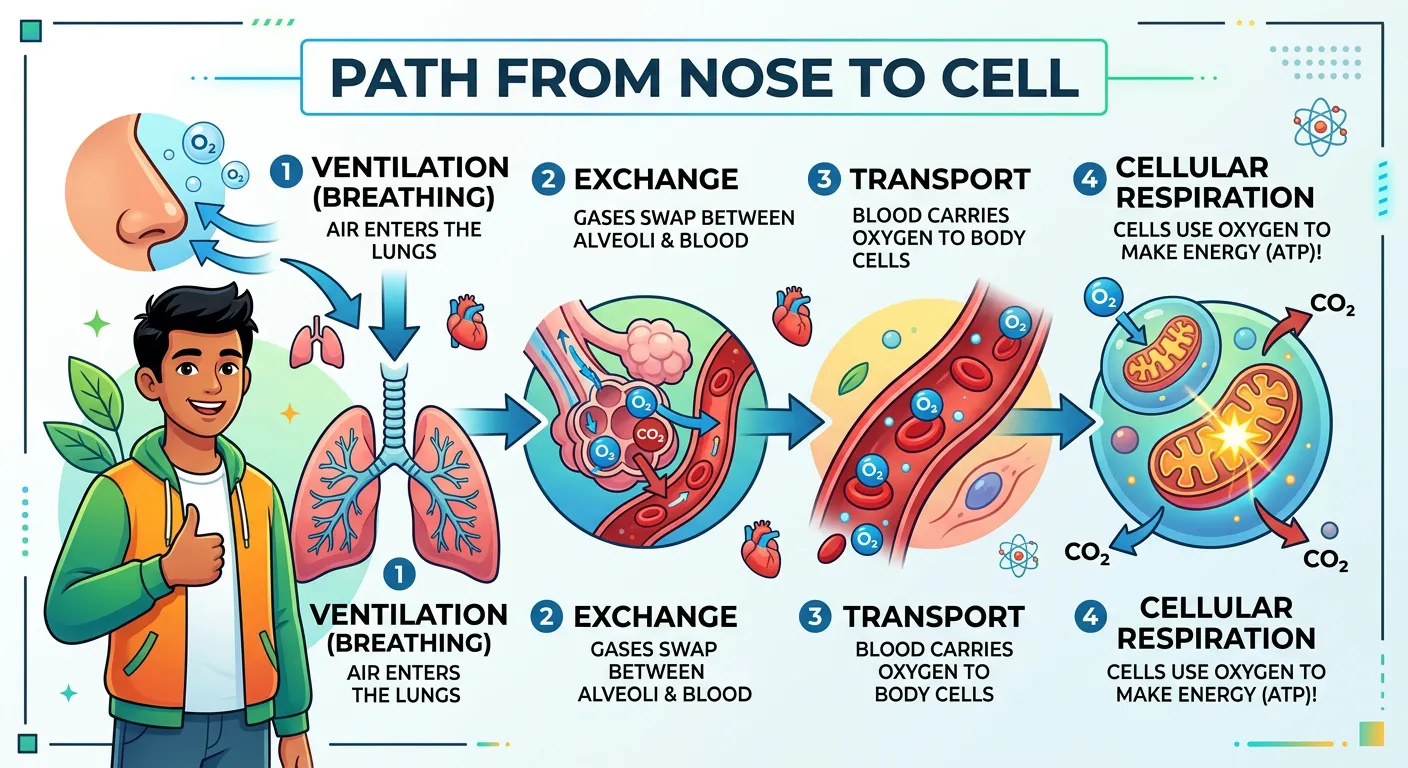
“Welcome, future doctors! Think of respiration as the ultimate energy-making factory. Just like your phone needs a battery charge, your cells need oxygen to produce ATP, the fuel for every movement. Today, we decode how air travels from your nose to your cells to keep you powered up!”
When we discuss the respiratory system in a NEET context, it is vital to distinguish between the mechanical act of breathing and the biochemical process of respiration. Breathing, or pulmonary ventilation, is simply the physical movement of air into and out of the lungs. However, the 'real' respiration happens at the cellular level. This is where oxygen acts as the ultimate electron acceptor in the mitochondrial electron transport chain. Without oxygen, the production of Adenosine Triphosphate (ATP) would grind to a virtual halt, leaving the body unable to power basic metabolic functions. Respiration is effectively a slow, controlled combustion process where glucose is oxidized to release energy, which is then 'packaged' into ATP molecules. This process is the biological equivalent of a power plant converting raw fuel into electricity.
In human physiology, we primarily focus on aerobic respiration because our high metabolic demand cannot be sustained by anaerobic pathways for long. While our muscles can briefly switch to lactic acid fermentation during intense exercise, this creates an 'oxygen debt' that must be repaid through heavy breathing after the activity ceases. For NEET aspirants, understanding the link between the respiratory system and cellular bioenergetics is crucial. You aren't just learning about lungs; you are learning how the body secures the raw materials for its energy currency. The efficiency of this system is staggering—aerobic respiration yields 36 to 38 ATP molecules per glucose molecule, compared to just 2 ATP in anaerobic conditions. This section serves as the foundation for understanding why any compromise in the respiratory tract leads to systemic failure—if the cells can't 'breathe' at the mitochondrial level, the organism cannot survive.
Quick Revision Points
- Breathing (Ventilation) is mechanical; Respiration (Cellular) is biochemical.
- Oxygen is the terminal electron acceptor in the Electron Transport Chain (ETC).
- ATP is the 'energy currency' generated primarily in the mitochondria via oxidative phosphorylation.
- Aerobic respiration yields significantly more energy (up to 19 times more) than anaerobic pathways.
- Carbon dioxide is the primary metabolic waste product of this energy production, which must be constantly removed to maintain pH balance.
NEET Exam Angle
- Focus on the distinction between 'Breathing' and 'Respiration' as they are often used interchangeably in lay terms but have specific biological definitions.
- Remember the chemical equation: C6H12O6 + 6O2 → 6CO2 + 6H2O + Energy (36-38 ATP).
- Understand that the rate of respiration is often regulated by the demand for ATP and the concentration of CO2 in the blood.
| Feature | Breathing (Ventilation) | Cellular Respiration |
|---|---|---|
| Level of Action | Organ system level (Lungs/Tract) | Cellular level (Mitochondria) |
| Nature of Process | Physical/Mechanical | Biochemical/Enzymatic |
| Energy Outcome | Consumes energy (muscle work) | Produces energy (ATP generation) |
| Primary Goal | Gas transport (O2 in, CO2 out) | Breakdown of nutrients for ATP |
02The Upper Respiratory Tract: Filtration, Humidification, and the Glottis Guard
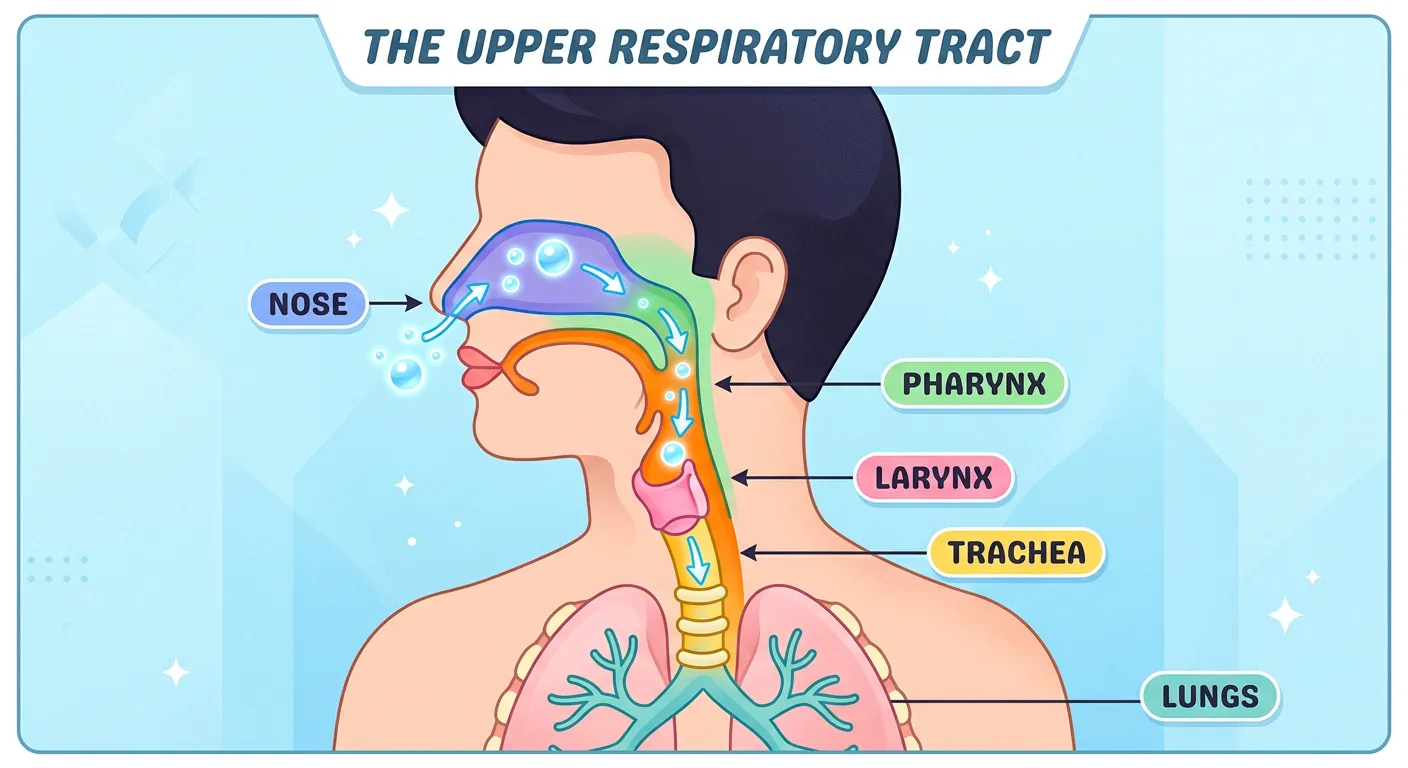
“Your journey begins at the nasal cavity, which acts like an air conditioner, warming and filtering the dust. Air then slides past the pharynx and larynx, our voice box. Think of the epiglottis as a smart traffic cop, preventing food from entering the windpipe. Safety first, always!”
The journey of air begins at the external nostrils (nares), leading into the nasal chamber. This isn't just a hollow pipe; it's a sophisticated air-conditioning unit. The nasal cavity is lined with pseudostratified ciliated columnar epithelium-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology)-class-11-neet-biology) and rich in goblet cells that secrete mucus. This mucus traps dust, pollen, and pathogens, while the cilia move the 'dirty' mucus toward the pharynx to be swallowed or expectorated. Furthermore, the extensive blood supply in the nasal mucosa warms the air to body temperature, and moisture is added to prevent the delicate lung tissues from drying out. This humidification is a critical step in maintaining the integrity of the lower respiratory system, as dry air can damage the alveolar membranes.
As air moves deeper, it reaches the pharynx, a common passage for both food and air. The pharynx is divided into three regions: the nasopharynx, oropharynx, and laryngopharynx. It leads into the larynx, or the 'voice box,' which is a cartilaginous box responsible for sound production. A high-yield point for NEET is the function of the epiglottis. During swallowing (deglutition), this thin, elastic cartilaginous flap covers the glottis—the opening of the larynx. This prevents food particles from entering the windpipe, acting as a 'traffic cop.' Any failure in this mechanism results in aspiration or choking. Understanding these anatomical safeguards helps students appreciate how the body manages complex dual-purpose pathways without cross-contamination. The larynx itself is supported by several cartilages, including the prominent thyroid cartilage (Adam's apple), the cricoid, and the arytenoid cartilages which assist in vocal cord tension.
Quick Revision Points
- Nasal lining: Pseudostratified ciliated columnar epithelium + Goblet cells.
- Functions of Nasal Cavity: Warming, Humidification, and Filtration (The 'Air Conditioning' effect).
- Pharynx: The junction where the digestive and respiratory systems meet; includes the Eustachian tube openings in the nasopharynx.
- Larynx: Cartilaginous structure involved in phonation; houses the vocal cords.
- Epiglottis: Prevents food entry into the larynx during swallowing; made of elastic cartilage.
NEET Exam Angle
- Questions frequently ask about the specific tissue type found in the respiratory lining.
- The 'Glottis vs. Epiglottis' distinction is a common trap in MCQ options; remember the glottis is the opening, and the epiglottis is the cover.
- Note that the larynx is made of nine cartilages (3 paired, 3 unpaired), though the primary focus remains on the Thyroid and Epiglottis.
- Understand that sound is produced by the vibration of vocal cords as air is expelled through the larynx.
03The Conducting Zone: Tracheal Architecture and the Bronchial Tree
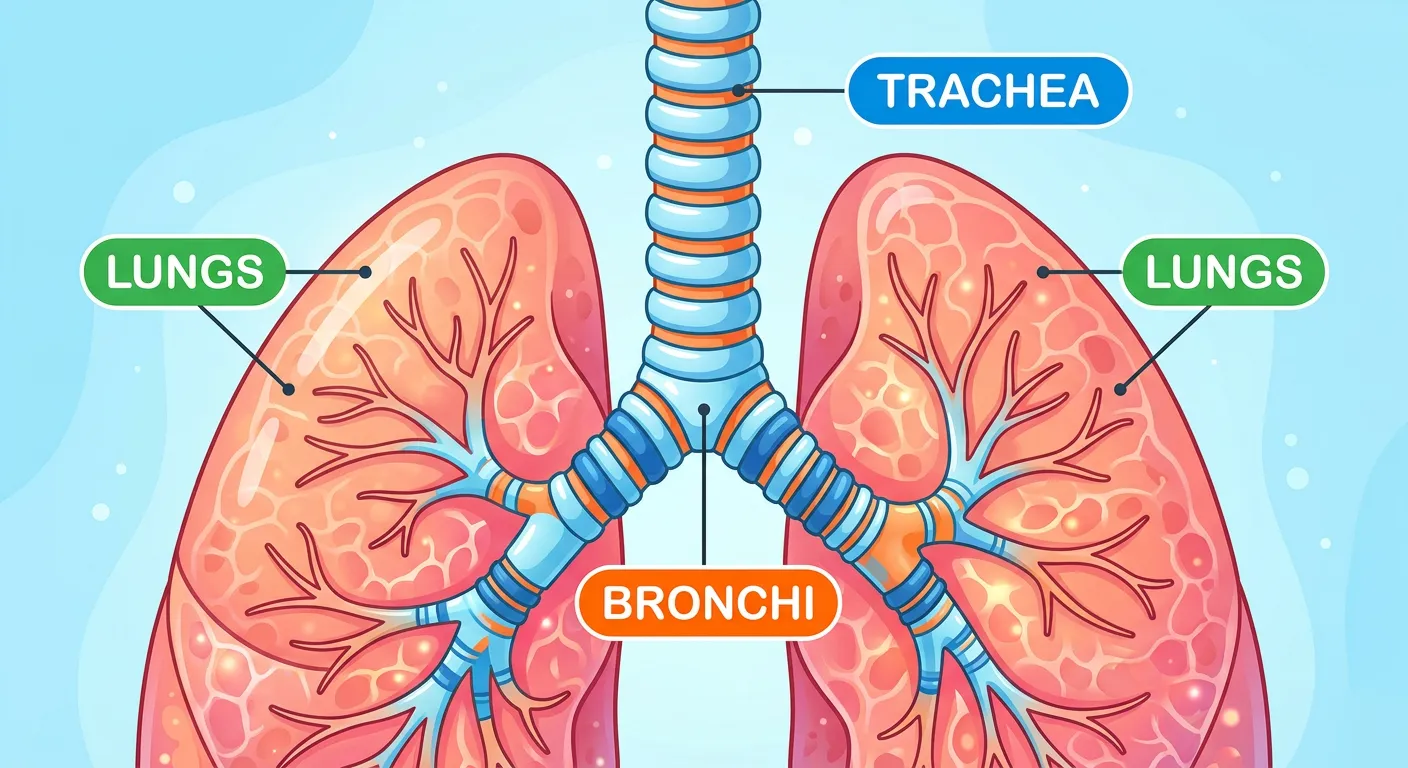
“Once past the larynx, air dives into the trachea, supported by C-shaped cartilage rings that act like a flexible vacuum hose. It then splits into two bronchi, heading into the left and right lungs. It's like a high-speed highway system delivering oxygen to every single corner.”
Past the larynx lies the trachea, a straight tube extending down to the mid-thoracic cavity. The most striking feature of the trachea is its support system: 16-20 C-shaped rings of hyaline cartilage. These rings are 'incomplete' posteriorly, meaning they don't form a full circle. This design is brilliant—it provides the structural rigidity needed to keep the airway open (patent) even under negative pressure during inspiration, while the soft posterior side allows the esophagus to expand slightly when you swallow a large bolus of food. Without these rings, your windpipe would collapse every time you took a deep breath or swallowed, much like a wet straw collapsing under suction.
At the level of the 5th thoracic vertebra (T5), the trachea divides into the right and left primary bronchi. These bronchi undergo repeated branching to form secondary and tertiary bronchi, eventually leading to very thin terminal bronchioles. This entire network—from the trachea to the terminal bronchioles—is known as the 'Conducting Zone.' Its primary job is to transport air, continue filtration, and add moisture. Crucially, no gas exchange occurs here. This gives rise to the concept of 'Anatomical Dead Space,' which is the volume of air (roughly 150ml in adults) that fills these passages but never reaches the alveoli for gas exchange. For NEET, remember that the cartilaginous support persists until the initial bronchioles but disappears as we reach the terminal ends, where smooth muscle takes over to regulate airflow through bronchoconstriction and bronchodilation.
Quick Revision Points
- Trachea branches at the level of the 5th Thoracic Vertebra (T5).
- Hyaline cartilage rings are C-shaped to prevent collapse and allow esophageal expansion.
- The conducting zone includes the trachea, bronchi, and terminal bronchioles.
- Dead Space: Air volume (~150ml) that stays in the conducting zone and does not participate in exchange.
- Cartilage support gradually decreases as the diameter of the bronchial tree narrows, eventually disappearing in bronchioles.
NEET Exam Angle
- Identify the specific vertebra (T5) where tracheal bifurcation occurs; this is a very high-frequency question.
- Understand the histological transition from ciliated epithelium to simpler cuboidal forms in the bronchioles.
- Be prepared for 'Assertion-Reason' questions regarding the incomplete nature of tracheal rings and the benefit of the posterior trachealis muscle.
04The Exchange Zone: Bronchioles and the Alveolar Blood-Gas Barrier
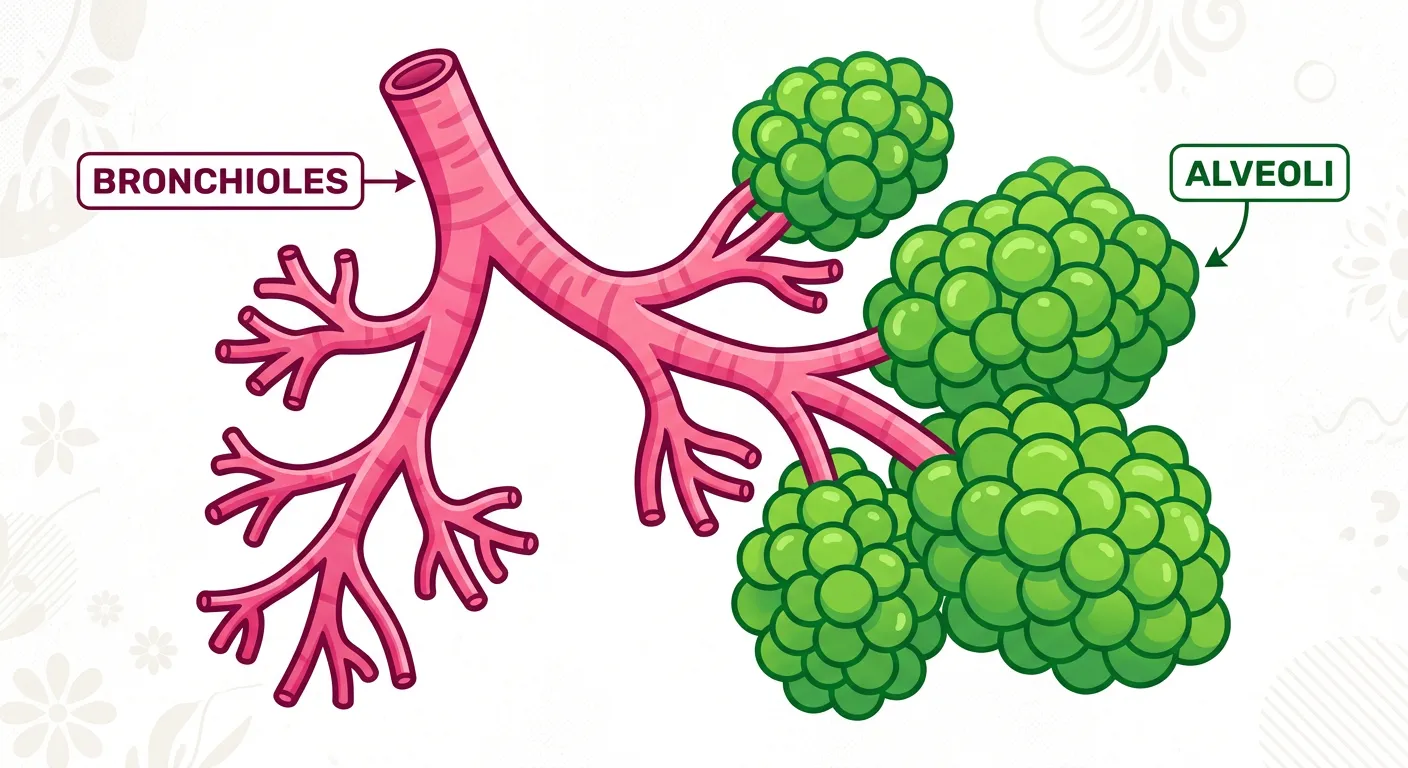
“Deep inside the lungs, bronchi branch into tiny twigs called bronchioles, ending in millions of tiny air sacs—the alveoli. These are the real MVPs! With their ultra-thin walls, they are the prime spot for gas exchange. Imagine billions of tiny balloons waiting to swap gas.”
The terminal bronchioles give rise to the 'Respiratory Zone,' which begins with the respiratory bronchioles and ends in the alveoli. The alveoli are the functional units of the lungs—tiny, vascularized bags where gas exchange actually occurs. To make exchange efficient, nature has maximized the surface area; the human lungs contain approximately 300 million alveoli, providing a total surface area nearly the size of a tennis court (70-100 square meters). This massive area is necessary to meet the high oxygen demands of a complex multicellular organism like a human, especially during physical exertion.
The alveolar wall is remarkably thin, composed primarily of Type I pneumocytes (specialized for exchange) and Type II pneumocytes. Type II cells are critical because they secrete surfactant (mainly lecithin/dipalmitoylphosphatidylcholine). This oily substance reduces surface tension within the alveoli, preventing them from collapsing (atelectasis) during expiration. The actual 'Respiratory Membrane'—the barrier air must cross to reach the blood—is less than 1 mm thick, usually around 0.2 to 0.5 micrometers. It consists of the squamous epithelium of the alveoli, the endothelium of the surrounding capillaries, and the fused basement membranes between them. This minimal thickness ensures that diffusion happens almost instantaneously, following the concentration gradient of gases from high partial pressure to low partial pressure.
Quick Revision Points
- Alveoli are the primary sites of gas exchange (the start of the Respiratory Zone).
- Type I Pneumocytes: Extremely thin squamous cells that facilitate gas diffusion.
- Type II Pneumocytes: Granular cuboidal cells that secrete surfactant to reduce surface tension.
- Surfactant prevents alveolar collapse and reduces the work required to expand the lungs.
- The respiratory membrane consists of three layers: Alveolar epithelium, Fused basement membrane, and Capillary endothelium.
NEET Exam Angle
- Focus on the components of the 'Diffusion Membrane' and its total thickness (<1mm).
- Recall the role of Lecithin as a major component of surfactant; its deficiency causes IRDS (Infant Respiratory Distress Syndrome) in premature infants.
- Understand that the exchange zone starts from the respiratory bronchioles, which have some alveoli in their walls, not the terminal bronchioles.
| Cell Type | Function | Key Feature |
|---|---|---|
| Type I Pneumocyte | Gas Exchange | Squamous, covers 95% of alveolar surface |
| Type II Pneumocyte | Surfactant Secretion | Cuboidal, contains lamellar bodies |
| Alveolar Macrophage | Immunity | 'Dust cells' that ingest foreign particles |
| Capillary Endothelial | Blood Containment | Simple squamous lining of the blood vessel |
05The Physics of Gas Exchange: Partial Pressure and Passive Diffusion
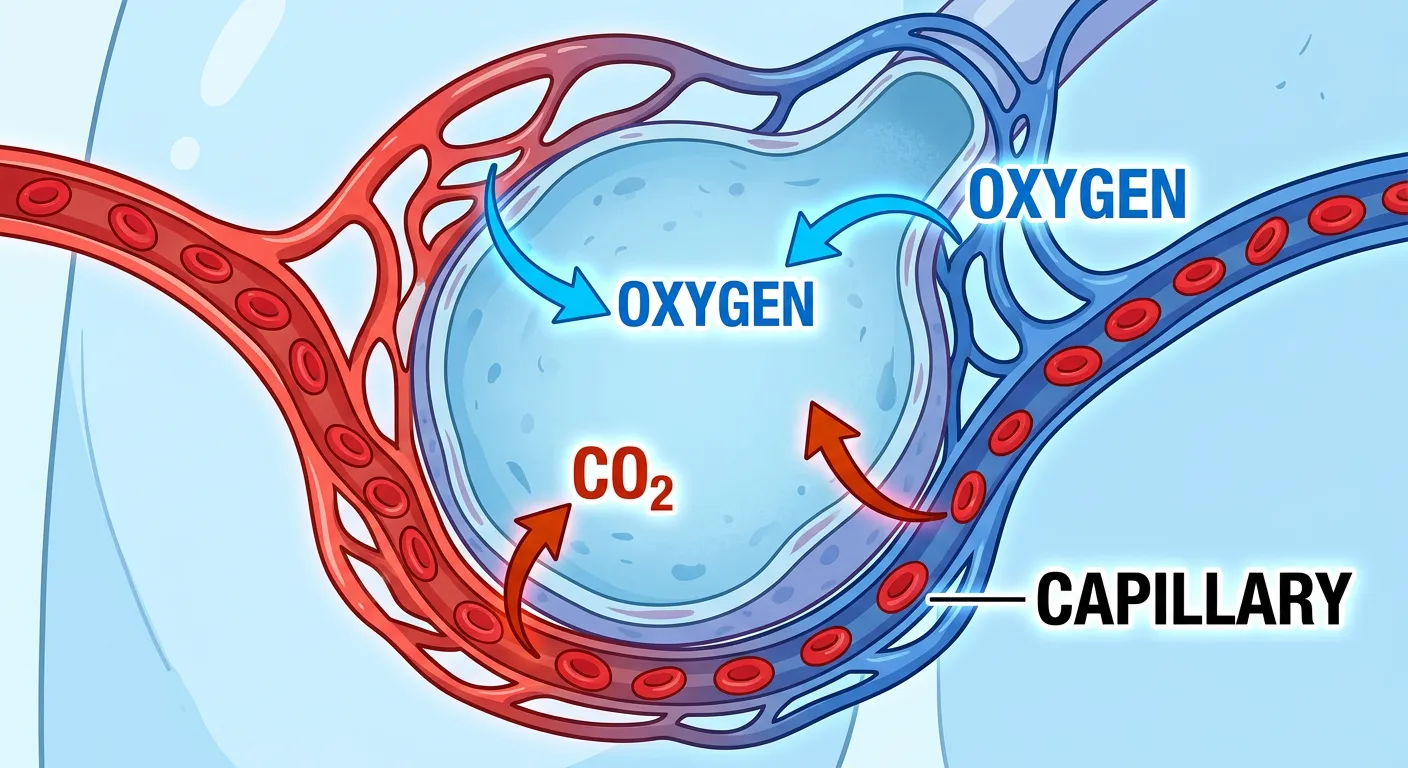
“This is where the magic happens! Oxygen jumps from the alveoli into the blood, while CO2 hitches a ride back out. It is a simple game of diffusion—moving from high concentration to low. No energy, no effort, just pure physics working for your body every second!”
Gas exchange in the lungs is a purely passive process governed by the laws of physics, specifically Dalton’s Law of Partial Pressures. A gas will always move from an area of higher partial pressure to an area of lower partial pressure. In the alveoli, the partial pressure of oxygen (pO2) is approximately 104 mm Hg, while in the deoxygenated blood arriving from the tissues via the pulmonary artery, it is only 40 mm Hg. This steep gradient 'pushes' oxygen across the respiratory membrane and into the blood. Conversely, the pCO2 is higher in the blood (45 mm Hg) than in the alveoli (40 mm Hg), causing CO2 to diffuse out for exhalation.
An interesting detail often tested in NEET is the solubility of gases. Carbon dioxide is 20-25 times more soluble in blood and biological membranes than oxygen. This means that even though the partial pressure gradient for CO2 (only 5 mm Hg) is much smaller than that for O2 (64 mm Hg), the rate of CO2 diffusion is still very high and efficient. Once oxygen enters the blood, it is quickly picked up by Hemoglobin (Hb) in red blood cells. This 'sequestering' of oxygen into oxyhemoglobin helps maintain the concentration gradient by keeping the amount of dissolved O2 in the plasma low, allowing more O2 to continue diffusing in from the alveoli. Factors like temperature, pH, and the thickness of the diffusion membrane also play critical roles in determining the net rate of exchange across the blood-gas barrier.
Quick Revision Points
- Diffusion is driven by partial pressure gradients (High to Low).
- pO2: Alveoli (104) > Oxygenated Blood (95) > Tissues (40).
- pCO2: Tissues (45) > Deoxygenated Blood (45) > Alveoli (40).
- CO2 is 20-25 times more soluble than O2, facilitating rapid exchange despite low pressure gradients.
- The respiratory membrane thickness and total surface area directly affect the diffusion capacity of the lungs.
NEET Exam Angle
- Memorize the specific partial pressure values for O2 and CO2 in Alveoli, Blood, and Tissues; these values are frequently used in matching-type questions.
- Understand how solubility affects the diffusion rate (CO2 vs O2 comparison).
- Recognize that no energy (ATP) is required for this gas exchange process; it is purely passive.
| Location | Partial Pressure of O2 (pO2) | Partial Pressure of CO2 (pCO2) |
|---|---|---|
| Atmospheric Air | 159 mm Hg | 0.3 mm Hg |
| Alveoli | 104 mm Hg | 40 mm Hg |
| Deoxygenated Blood | 40 mm Hg | 45 mm Hg |
| Oxygenated Blood | 95 mm Hg | 40 mm Hg |
| Tissues | 40 mm Hg | 45 mm Hg |
06Mechanism of Ventilation: Boyle’s Law and the Diaphragmatic Pulse
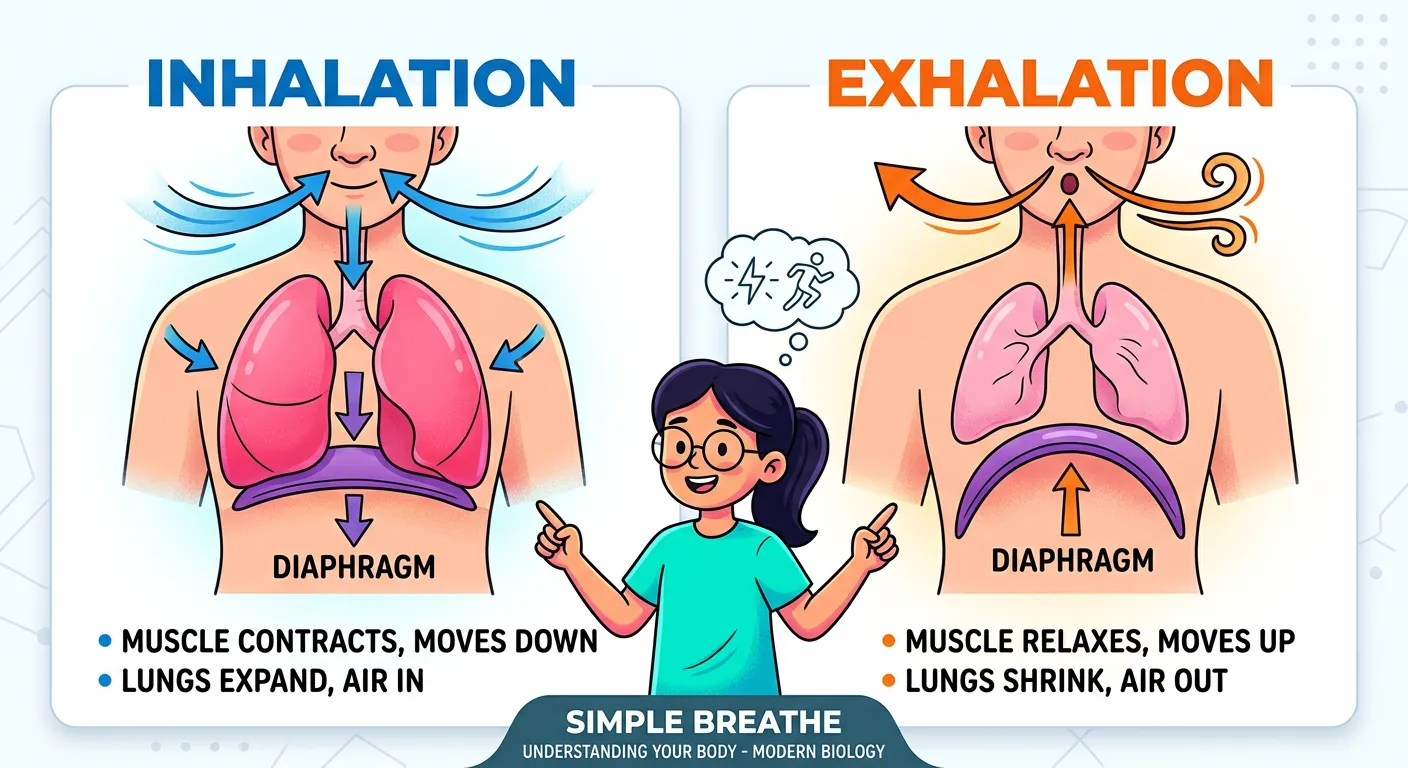
“How do we breathe? Meet the diaphragm, the muscle floor of your chest. When it pulls down, your chest cavity expands, and air rushes in like a vacuum. When it relaxes, it pushes up, and air is squeezed out. It is the rhythmic dance that sustains your life!”
Human breathing operates on the principle of negative pressure ventilation. According to Boyle’s Law, the pressure of a gas is inversely proportional to its volume ($P \propto 1/V$). To draw air in (Inspiration), we must increase the volume of our thoracic cavity. This is achieved by two primary muscle groups: the diaphragm and the external intercostal muscles. The thoracic cavity acts as an airtight chamber, and any change in its volume is mirrored by the lungs. When the diaphragm contracts, it flattens and moves downward, increasing the vertical volume of the chest. Simultaneously, the external intercostals contract, lifting the ribs and sternum upward and outward (often described as 'pump-handle' and 'bucket-handle' movements), which increases the dorso-ventral volume. As the total thoracic volume increases, the intra-pulmonary pressure drops to about -2 mm Hg relative to atmospheric pressure, and air rushes in from the outside.
In contrast, quiet expiration is largely a passive process. When these muscles relax, the diaphragm returns to its dome shape and the rib cage falls back to its original position due to elastic recoil. This decreases the thoracic volume, causing the internal pressure to rise above atmospheric pressure (about +2 mm Hg), which forces the air out. Throughout this cycle, the double-layered pleura plays a vital role. The pleural fluid between the parietal and visceral layers reduces friction and creates surface tension that keeps the lungs 'stuck' to the chest wall. This ensures they expand whenever the chest cavity does. During forceful breathing, such as exercise or blowing a whistle, accessory muscles like the abdominal muscles and internal intercostals are recruited to actively pull the ribs down and push the diaphragm up, making the process active and much more rapid. This mechanical integration of muscles, bones, and pressure gradients is what allows us to adapt our breathing to various physiological needs.
Quick Revision Points
- Inspiration: Active process; diaphragm and external intercostals contract to increase volume.
- Expiration: Passive process (during quiet breathing); muscles relax, allowing elastic recoil.
- Boyle’s Law: Increased thoracic volume leads to decreased intra-pulmonary pressure.
- Pleural fluid: Lubricates lung movement and provides the 'grip' for lung expansion.
- Forced breathing: Involves abdominal muscles and internal intercostals to aggressively reduce volume.
NEET Exam Angle
- Distinguish between 'Inspiration' (active) and 'Normal Expiration' (passive) carefully in MCQs.
- Remember that the diaphragm contributes about 75% of the volume change during quiet breathing; it is the most important respiratory muscle.
- Understand that internal intercostals and abdominal muscles are only used during forced expiration (e.g., blowing out a candle) and not during normal quiet breathing.
- The negative pressure in the pleural cavity (intra-pleural pressure) is essential to keep the lungs from collapsing.
07Summary and NEET Essentials: Respiratory Volumes and System Integration
“So, we have mastered the path: nose, trachea, alveoli, and blood. You now understand how we ventilate and exchange gases. Keep this flow chart in mind, and you will ace those NEET questions on respiratory volumes and disorders. Stay curious, study smart, and keep breathing easy!”
To master the respiratory system for NEET, one must be proficient in 'Spirometry'—the measurement of lung volumes and capacities. Tidal Volume (TV) is the standard 500ml moved during quiet breathing. However, we have significant reserves: the Inspiratory Reserve Volume (IRV) is the extra air we can inhale (2500-3000ml), and the Expiratory Reserve Volume (ERV) is the extra air we can exhale (1000-1100ml). A critical concept is the Residual Volume (RV)—the air that remains in the lungs even after the most forceful expiration. You can never truly 'empty' your lungs; if you did, the alveoli would collapse and stick together. These volumes are often combined to define 'Capacities,' like Vital Capacity (VC), which is the total exchangeable air, and Total Lung Capacity (TLC), which is the sum of all volumes.
Finally, we must touch upon respiratory health and disorders, which are high-yield topics. Disorders like Asthma involve the inflammation of bronchi and bronchioles, causing bronchospasms and wheezing. Emphysema, often caused by chronic smoking, is a condition where alveolar walls are damaged, drastically reducing the total surface area for gas exchange and making expiration difficult. Occupations involving stone-breaking, silica, or asbestos can lead to fibrosis (occupational respiratory disorders) where lung tissue becomes scarred and loses elasticity. In your NEET preparation, treat the respiratory system as an integrated whole—connecting the anatomy of the tubes to the physics of the air and the clinical reality of the diseases. Understanding how oxygen is carried by hemoglobin and how CO2 is transported primarily as bicarbonate ions is the final piece of this physiological puzzle.
Quick Revision Points
- Tidal Volume (TV): ~500 ml; about 350ml reaches the alveoli.
- Vital Capacity (VC) = TV + IRV + ERV; it represents the max air you can move.
- Residual Volume (RV) cannot be measured by a simple spirometer because it never leaves the lungs.
- Asthma: Characterized by inflammation and bronchospasm leading to breathing difficulty.
- Emphysema: Permanent alveolar wall damage; decreased surface area and loss of lung elasticity.
- Occupational Disorders: Fibrosis due to chronic dust inhalation (Silicosis/Asbestosis).
NEET Exam Angle
- Practice calculating capacities (e.g., TLC, FRC, VC) from given volumes; these are common numerical problems.
- Focus on the definitions of disorders, specifically the 'reduced surface area' aspect of Emphysema and the 'fibrosis' aspect of occupational diseases.
- Note that Residual Volume (RV) is always present to prevent lung collapse and allow for continuous gas exchange even between breaths.
| Volume/Capacity | Definition | Approx. Value (Adult Male) |
|---|---|---|
| Tidal Volume (TV) | Normal breath | 500 ml |
| Inspiratory Reserve (IRV) | Extra air inhaled forcefully | 2500 - 3000 ml |
| Residual Volume (RV) | Air left after max exhale | 1100 - 1200 ml |
| Vital Capacity (VC) | Max air exhaled after max inhale | 3500 - 4500 ml |
| Total Lung Capacity (TLC) | Total air in lungs after max inhale | 5000 - 6000 ml |
Recommended Reading
Explore related Biology topics to build deeper chapter connections for NEET.
- Morphology and Modifications · Topic 2.1
- Families · Topic 2.10
- Animal Tissues · Topic 2.11
- Frog Morphology · Topic 2.12
- Digestive System · Topic 2.13
- Circulatory System · Topic 2.14
- Jump to Key Terms (Quick Revision)
- Review Common NEET Mistakes
- Read Topic FAQs
- Check PYQ Pattern Notes
- Practice NEET MCQs
- Solve NEET PYQs
📚 Key Terms
⚠️ Common NEET Mistakes
- 1Confusing the terminal bronchioles (end of conducting zone) with respiratory bronchioles (start of exchange zone).
- 2Assuming that expiration is always an active process; in normal quiet breathing, it is actually passive due to elastic recoil.
- 3Thinking that the tracheal rings are complete circles; they are C-shaped and open at the back to allow for esophageal expansion.
- 4Believing that all air is expelled from the lungs during forced expiration; Residual Volume always remains to prevent alveolar collapse.
- 5Using the terms 'breathing' and 'respiration' interchangeably in a technical exam context; they refer to different levels of the process.
📝 NEET PYQ Pattern
Between 2018–2024, NEET questions have frequently targeted the 'Mechanism of Breathing' and 'Respiratory Volumes'. Specifically, students should focus on the site of gas exchange (Alveoli) and the muscles involved in inspiration/expiration, as these appear in 40% of the unit-specific questions. Additionally, the definition of Emphysema and calculations of Vital Capacity are recurring favorites.
❓ Frequently Asked Questions
What is the specific role of the C-shaped cartilaginous rings in the human trachea?
The C-shaped cartilaginous rings, made of hyaline cartilage, provide structural support to the trachea. They prevent the airway from collapsing during the negative pressure changes of inspiration. Their 'C' shape (incomplete posteriorly) allows the esophagus, which sits behind the trachea, to expand during swallowing.
How does the partial pressure of Oxygen (pO2) change from the alveoli to the systemic tissues?
In the alveoli, pO2 is high (~104 mm Hg). It diffuses into the blood, resulting in oxygenated blood with a pO2 of ~95 mm Hg. When this blood reaches the systemic tissues where pO2 is low (~40 mm Hg), oxygen diffuses out of the blood and into the cells to support aerobic respiration.
Why is the epiglottis referred to as a 'traffic cop' in the respiratory system?
The epiglottis is a cartilaginous flap that acts as a switch. During normal breathing, it stays open to allow air into the larynx. During swallowing, it covers the glottis (the opening of the larynx) to ensure that food and liquids are directed into the esophagus and do not enter the respiratory tract.
What is the difference between the conducting zone and the respiratory zone?
The conducting zone (nose to terminal bronchioles) is responsible for transporting, filtering, warming, and humidifying air but does not perform gas exchange. The respiratory zone (respiratory bronchioles to alveoli) is the actual site where oxygen and carbon dioxide are exchanged between the air and the blood.
How does the diaphragm facilitate inspiration according to Boyle's Law?
Boyle's Law states that as volume increases, pressure decreases. When the diaphragm contracts and moves downward, it increases the volume of the thoracic cavity. This leads to a decrease in intra-pulmonary pressure below atmospheric pressure, causing air to be 'sucked' into the lungs.
Why is Carbon Dioxide diffusion more efficient than Oxygen diffusion across the respiratory membrane?
Even though the partial pressure gradient for CO2 is much smaller than for O2, CO2 is 20-25 times more soluble in the blood and the aqueous layers of the respiratory membrane. This high solubility allows CO2 to diffuse rapidly across the barrier.
Written By
NEET Content Strategist & Biology Expert
Sangita Kumari is a NEET educator and content strategist with over 6 years of experience teaching Biology, Chemistry, and Physics to Class 11 and 12 aspirants. She helps bridge the gap between traditional NCERT preparation and modern AI-powered learning. Her content is trusted by thousands of NEET aspirants across India.